The rehab journey of Kris – by Leira Pamp, Student Placement
For 6 weeks, I was on placement as a student physiotherapist with Neurotherapy Worx, where I have been introduced to various Tecnobody technologies, such as their D-Wall, Prokin, and the most recent addition to Neurotherapy Worx’s offerings – the Walker View.

Technobody Rehab Equipment
For the uninitiated, the Tecnobody kit is made primarily for use in a commercial or small group training environment, but it also has fantastic benefits in rehab facilities, such as with the neurological patients I have been seeing on placement. The D-Wall, for example, utilises a 3D camera embedded in the TV wall, which with information about the client such as their height and weight, can track their movements to create interactive challenges such as catching imaginary balls in a safer environment. It also utilises force plates, to allow you to see how the user bears weight. This means you can make adjustments to their posture and positioning in real time, while giving them something visual to help reinforce what you are saying.
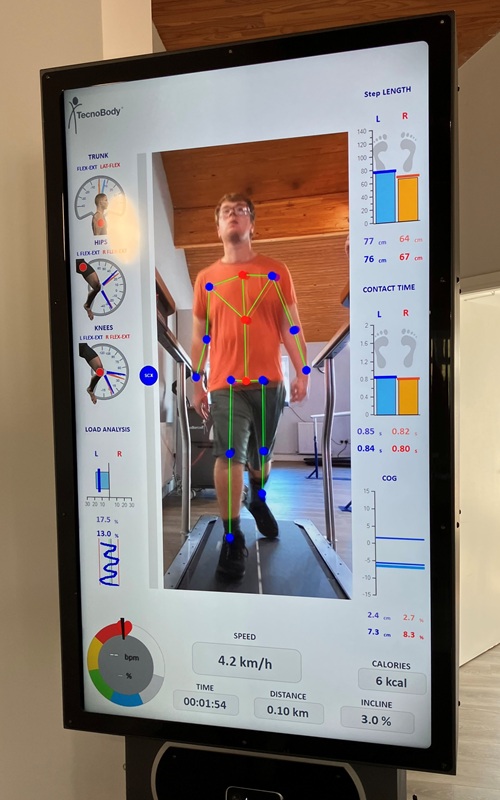
The Walker View is a treadmill that utilises the same 3D camera technology as the D-Wall to analyse everything about a person’s movement. With the only initial measurements needed being the patient’s height and weight, a simple 2-minute gait analysis can tell you data such as the person’s degrees of trunk flexion, extension, and lateral flexion while walking. It also shows you their knee and hip ranges of movement, their step height, and stride length, which gives the physiotherapist objective measures about how the patient is walking. The videos and data are also saved on the client’s account, making it easy to scroll through the video to see the real time results as well as the overview you are given at the end.
Client Profile
One patient I have seen on this placement is Kris. Kris is patient who was hit by a car at a very young age, suffering a fractured skull and pelvis, and was diagnosed with severe brain damage after being in a coma in hospital. As a result of his injuries, he had to relearn key skills, such as walking, talking, and tasks that require coordination between different areas of the body, such as eating. As a result of his brain injury, Kris must wear an articulated ankle foot orthosis (AFO) on his right foot, which has been 3D printed for him. The nature of the orthosis being 3D printed means the patient is able to increase the heel block on the AFO at regular intervals to encourage a better tibial shaft angle, as the patient tolerates.
The reason for collecting and comparing this data is try to encourage Kris to wear his AFO more regularly. Kris’s goal is to improve the appearance of his gait, as he currently mobilises with his right leg in a more externally rotated position compared to the left. Prior to the data collection and interpretation, the patient predominantly wore his old insoles with regular trainers. He had worn his new ones for a weekend abroad, but as he spent the entire weekend in them, he began to struggle to tolerate the new ones. His AFO he would tolerate for a few hours a day when out and about, but cannot achieve a full day in it.
Data Collection & Analysis
The data in the poster above was gathered across two appointments. The old insoles, new insoles, and AFO were collected on the same day, while the increased heel on the AFO was taken at the second appointment. There was also data collected surrounding the patient’s trunk ranges of movement, from flexion to extension and lateral flexion, but I have opted to leave these off the poster as there was only minimal differences between the different interventions. It is important to note as well, in the AFO with increased heel height, the patient was walking faster and tried to jog. This means some of the data, such as the contact time, appears to have had a negative effect, when it was actually the nature of the patient’s movement being different.
When looking at the data collected, there are some subtle differences, but it largely moves in the right direction. When comparing the old insoles to the use of the AFO, the patient shows an increase in right hip flexion, and a decrease in left hip flexion. The decrease in left hip flexion may be due to the patient no longer having to work as hard when using his left leg. When you compared this to the AFO with the increased heel height, we actually have an increase in flexion in both hips, though this may also be due to the fact the patient was jogging during this trial, so had to move faster, necessitating him bringing his feet up higher.
The patient’s right leg step length increased by 1.5inches when comparing the initial value of old insole to increased heel height AFO. This is this is likely due to the AFO providing more stability to the patient’s foot when in the toe off phase of gait, allowing the patient to extend his hip further back before stepping through.
The biggest improvement across all interventions is the patient’s increase in knee flexion when comparing his old insoles to his AFO with heel increase. As is shown on the poster, the patient experienced a 49% increase in his right knee flexion, as the AFO allowing the patient to have more stability in the toe off phase meant the patient had to bend his hip and knee more in order to achieve a full heel strike.
The Walker View does come with additional monitors that can be attached to the patient’s footwear, making it easier to monitor their movements through the gait cycle. When these have been added to the clinic, they will be an invaluable resource for continuing to progress patients such as Kris. Through using the articulated AFO, Kris was able to achieve a fast jog for the first time post brain injury. This has then inspired Kris’s new goal, of running up Darwen Tower.
The results we gained from Kris’ use of the articulated AFO also follow a similar pattern to research being conducted for different types of brain injuries, comparing static vs articulated AFOs. A study from Vieira de Paula, et al., (2024) utilised home-based mobility training for 30 minutes per day, over a period of four weeks, in individuals who had had a stroke. The results postulated that the articulated group showed greater improvement both with the outcome measure (timed up and go), but also with their functional ability to complete tasks within their home environment. While it didn’t directly have any impact on the patients’ mental health scores at this time, their improved mobility and ability to complete tasks around the home independently may improve these values over time, as it allows the patient to regain independence they may have lost after their brain injury.

In conclusion, I believe this technology will be a great addition to the clinic at Neurotherapy Worx, as it allows patients to see what the therapist sees, which encourages them to make changes in real time with each repeated trial. For this particular patient, the articulated AFO is making a big difference to his ability to mobilise how he wants to, to help him achieve goals he did not realise were possible for him.
Paula, G. V. de, Luvizutto, G. J., Miranda, L. A., Regina da Silva, T., Silva, L. T. C., Winckler, F. C., Modolo, G. P., Chiloff, C. L. M., Bazan, S. G. Z., Molle da Costa, R. D., Martin, L. C., Bazan, R. (2024). Articulated ankle-foot orthoses associated with home-based task-specific training improve functional mobility in patients with stroke: a randomized clinical trial. Topics in Stroke Rehabilitation, 1–14. https://doi.org/10.1080/10749357.2024.2399467